Chart Documentation: A Complete Information to Correct and Efficient Medical Report Maintaining
Associated Articles: Chart Documentation: A Complete Information to Correct and Efficient Medical Report Maintaining
Introduction
On this auspicious event, we’re delighted to delve into the intriguing matter associated to Chart Documentation: A Complete Information to Correct and Efficient Medical Report Maintaining. Let’s weave fascinating data and provide contemporary views to the readers.
Desk of Content material
Chart Documentation: A Complete Information to Correct and Efficient Medical Report Maintaining
.png)
Medical charts function the cornerstone of affected person care, offering a chronological document of a affected person’s well being journey. Correct and complete chart documentation is essential for efficient communication amongst healthcare professionals, making certain continuity of care, facilitating applicable remedy selections, and defending each sufferers and suppliers from authorized dangers. This text explores important pointers for chart documentation, emphasizing readability, completeness, accuracy, and adherence to authorized and moral requirements.
I. Elementary Ideas of Chart Documentation:
Efficient chart documentation hinges on a number of key rules:
-
Accuracy: All entries should be factual, goal, and free from subjective opinions or interpretations. Use exact medical terminology and keep away from jargon or abbreviations that is likely to be misunderstood. If an error happens, right it appropriately, by no means erase or obliterate the unique entry. As an alternative, draw a single line via the inaccurate data, preliminary it, and date the correction.
-
Completeness: The chart ought to comprise all related data pertaining to the affected person’s well being standing, remedy, and response to care. This consists of the affected person’s medical historical past, present complaints, bodily examination findings, diagnostic check outcomes, remedy plans, medicines administered, and the affected person’s progress. Omitting vital data can result in misdiagnosis, remedy errors, and compromised affected person security.
-
Timeliness: Entries needs to be made promptly after the occasion or evaluation. Delayed documentation can result in incomplete or inaccurate information, hindering the flexibility to trace the affected person’s progress and make knowledgeable selections. Ideally, documentation ought to happen instantly following affected person interplay.
-
Readability and Legibility: Make sure that all entries are legible, well-organized, and simply comprehensible. Use clear and concise language, avoiding ambiguous phrases or phrases. Correct grammar and spelling are important. If utilizing abbreviations, guarantee they’re standardized and broadly understood inside the healthcare setting.
-
Objectivity: Give attention to observable info and measurable knowledge. Keep away from subjective opinions or private judgments. As an alternative of writing "affected person seems anxious," doc observable behaviors equivalent to "affected person exhibiting speedy coronary heart fee, elevated respirations, and fidgeting."
-
Confidentiality: All data contained inside the medical chart is strictly confidential and guarded by legislation (e.g., HIPAA within the US). Entry to the chart needs to be restricted to approved personnel solely. Preserve affected person privateness always, each in written and digital information.
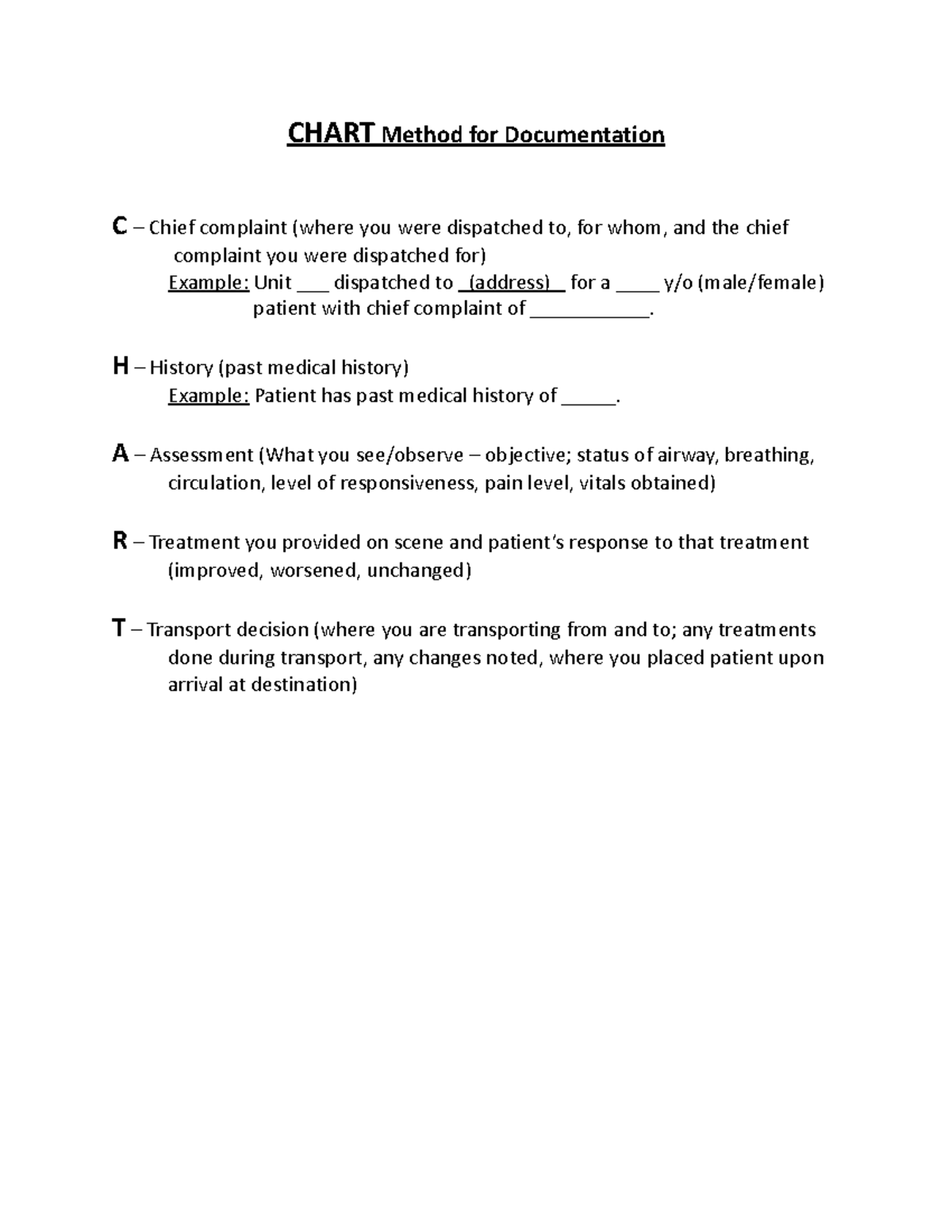
II. Particular Components of Chart Documentation:
Efficient chart documentation encompasses varied parts:
-
Affected person Identification: Start every entry with the affected person’s full identify, date of delivery, medical document quantity, and date and time of the entry.
-
Chief Grievance: Clearly state the rationale for the affected person’s go to within the affected person’s personal phrases, every time potential.
-
Historical past of Current Sickness (HPI): Present an in depth account of the affected person’s present sickness, together with the onset, period, character, location, severity, and any related signs. Use the mnemonic SOCRATES (Website, Onset, Character, Radiation, Related signs, Timing, Exacerbating/relieving elements, Severity) to make sure complete documentation.
-
Previous Medical Historical past (PMH): Doc the affected person’s previous diseases, surgical procedures, hospitalizations, allergic reactions, and present medicines.
-
Household Historical past (FH): Word any vital medical situations current within the affected person’s members of the family.
-
Social Historical past (SH): Embrace related social elements equivalent to smoking, alcohol consumption, drug use, occupation, and dwelling scenario.
-
Assessment of Programs (ROS): Systematically overview every physique system to determine any signs or abnormalities.
-
Bodily Examination (PE): Report goal findings from the bodily examination, together with important indicators, basic look, and findings from particular physique techniques.
-
Diagnostic Checks and Procedures: Doc all diagnostic exams carried out, together with the outcomes and interpretations.
-
Therapy Plan: Clearly define the deliberate remedy, together with medicines, therapies, and procedures.
-
Progress Notes: Recurrently doc the affected person’s progress, response to remedy, and any modifications of their situation. Use a structured format (e.g., SOAP – Subjective, Goal, Evaluation, Plan) to make sure consistency.
-
Discharge Abstract: Upon discharge, summarize the affected person’s hospital course, analysis, remedy acquired, and plan for continued care.
III. Authorized and Moral Concerns:
Correct and full chart documentation is just not solely important for affected person care but additionally essential for authorized and moral causes:
-
Authorized Safety: Effectively-documented charts can defend healthcare suppliers from malpractice claims by demonstrating that applicable care was offered. Conversely, incomplete or inaccurate documentation can be utilized towards suppliers in authorized proceedings.
-
Continuity of Care: Correct documentation facilitates seamless transitions of care between completely different healthcare suppliers and settings. This ensures that sufferers obtain constant and coordinated care.
-
Compliance with Rules: Healthcare suppliers should adhere to varied rules and requirements relating to medical document protecting. These rules fluctuate by nation and jurisdiction however typically embody necessities for confidentiality, knowledge safety, and document retention.
-
Moral Obligations: Healthcare professionals have an moral obligation to take care of correct and full medical information. It is a elementary side of offering accountable and patient-centered care.
IV. Digital Well being Information (EHRs):
The widespread adoption of EHRs has revolutionized medical document protecting. Whereas EHRs provide quite a few advantages, together with improved entry to data and lowered paperwork, additionally they current distinctive challenges for documentation:
-
Knowledge Safety: EHRs comprise delicate affected person data, requiring strong safety measures to guard towards unauthorized entry and knowledge breaches.
-
Template Use: Whereas templates can streamline documentation, they shouldn’t be used to interchange considerate and individualized entries. Make sure that all related data is included, even when it requires deviating from the template.
-
Copy and Paste Performance: Keep away from extreme use of the copy and paste operate, as this may result in inaccurate or outdated data. All the time overview and confirm the accuracy of any copied data.
-
Authentication and Signatures: Make sure that all entries are correctly authenticated and electronically signed to take care of accountability and forestall unauthorized modifications.
V. Enhancing Chart Documentation Practices:
A number of methods can improve the standard of chart documentation:
-
Common Coaching: Healthcare professionals ought to obtain common coaching on correct documentation strategies and updates on related rules and pointers.
-
Use of Standardized Terminology: Using standardized medical terminology ensures consistency and readability throughout the healthcare system.
-
Common Chart Audits: Conducting common audits of medical information can determine areas for enchancment and guarantee adherence to established pointers.
-
Suggestions Mechanisms: Set up mechanisms for suggestions on documentation practices, permitting for steady enchancment and identification of areas needing consideration.
-
Implementation of Documentation Insurance policies and Procedures: Develop clear and concise insurance policies and procedures for chart documentation, making certain all workers members perceive and comply with the established pointers.
VI. Conclusion:
Correct and complete chart documentation is a vital side of offering high-quality affected person care. Adhering to established pointers, sustaining moral requirements, and using greatest practices for digital document protecting are important for making certain the integrity and reliability of medical information. By prioritizing correct, full, and well timed documentation, healthcare professionals can contribute to improved affected person security, efficient communication, and the general high quality of care. Steady training and a dedication to greatest practices are essential for sustaining the very best requirements of medical document protecting.





Closure
Thus, we hope this text has offered invaluable insights into Chart Documentation: A Complete Information to Correct and Efficient Medical Report Maintaining. We hope you discover this text informative and helpful. See you in our subsequent article!